

Common Reasons Clinical Trial Sites Fail Sponsor Feasibility Evaluation
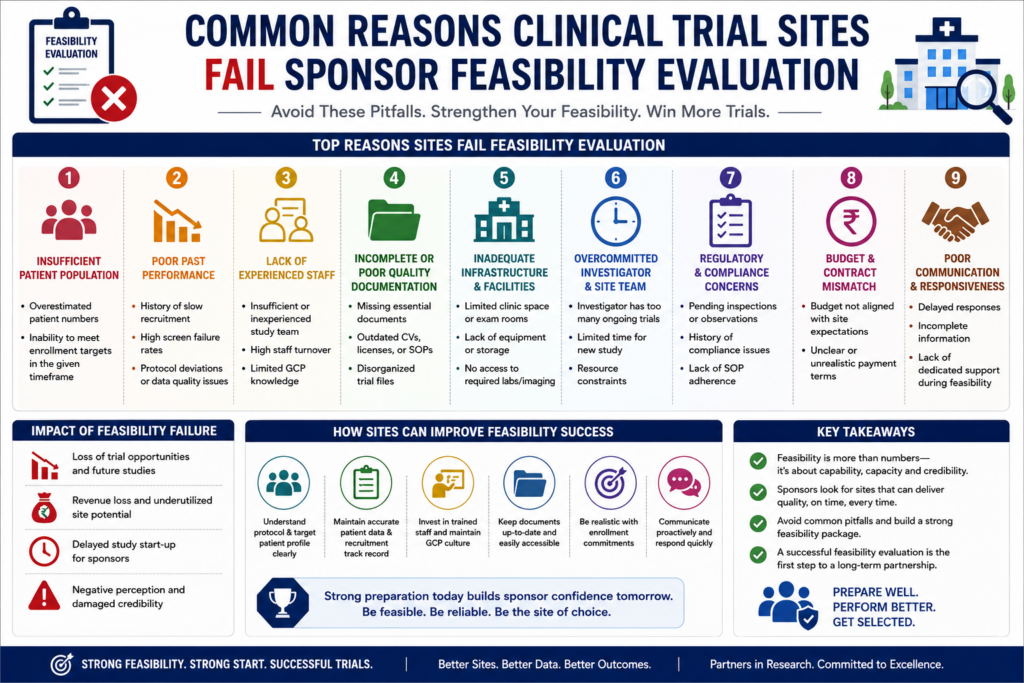
Clinical Trial Feasibility Failure.. Three months into a Phase III global trial, a sponsor realized that their lead site in India—selected for its high patient volume—had not enrolled a single subject. The Investigator was a high-profile KOL with five other active trials. The site staff was overwhelmed, the Ethics Committee (EC) had an unexpected three-month backlog, and the storage facility for Investigational Product (IP) lacked temperature-controlled backup. This failure cost the sponsor approximately $45,000 in lost startup costs and delayed the regional database lock by twelve weeks. In fifteen years of clinical operations, I have seen that high-quality data and timeline adherence do not happen by accident. They are the result of looking past the “paper feasibility” and assessing the site’s actual capacity to execute under the New Drugs and Clinical Trials Rules (2019). Executive Summary for Sponsors and CROs Feasibility failure is the single largest controllable risk to trial timelines and budgets. When a site fails feasibility or, worse, passes feasibility but fails execution, the financial impact is compounding. Beyond the $30,000 to $50,000 spent on administrative startup, monitoring, and IP logistics, the second-order effects include missed milestones and compromised data integrity. A successful feasibility evaluation in the Indian landscape requires a granular understanding of institutional bureaucracy, PI commitments, and patient pathways. Sponsors must move away from generic questionnaires and focus on evidence-based site selection that prioritizes ALCOA+ principles and regulatory readiness. The Reality of the Approval Process in India Many sponsors assume that a quick feasibility turnaround translates to a quick startup. This is rarely the case. Sites often fail feasibility because they cannot clearly map out their internal approval timelines. A site might claim a 30-day startup, but if they have an unorganized Institutional Ethics Committee (IEC) that only meets once every two months, that timeline is impossible. Furthermore, the mandatory registration on the Clinical Trials Registry – India (CTRI) requires specific documentation that many sites fail to prepare in advance. Operational delays frequently occur at the intersection of legal and administrative review. If a site’s legal department is notorious for 6-month turnaround times on Clinical Trial Agreements (CTAs), the site is a failure for any trial requiring rapid enrollment. Critical Operational Bottlenecks Sites fail feasibility when they lack a dedicated Study Coordinator or when the PI delegates too much responsibility to junior residents with high turnover rates. During a site assessment, the presence of a calibrated centrifuge or a -20°C freezer is basic. What matters is the maintenance log, the power backup protocol, and the staff’s understanding of “Source Data.” If a site cannot demonstrate a clear workflow for data entry into the Electronic Data Capture (EDC) system within 24–48 hours, they will become a bottleneck during the trial. Site failures also stem from a lack of “Patient Depth.” A site may have 500 patients with a specific condition, but if 90% of those patients live more than 200 kilometers away and the protocol requires weekly visits, the feasibility of recruitment is near zero. Case Studies in Feasibility and Execution Failure Case Study 1: The “Ghost” Principal Investigator Study Type: Phase II Oncology Site Type: Large Private Multi-specialty Hospital Problem: Zero recruitment after 4 months of activation. Root Cause: The PI was listed on six other trials and delegated all screening to a junior fellow who did not understand the inclusion/exclusion criteria. Action Taken: Site was closed after the first monitoring visit. Outcome: $60,000 loss in startup and IP costs. Lesson Learned: Always evaluate the PI’s “Time-on-Study” and the number of competing protocols currently active at the site. Case Study 2: Regulatory and Equipment Collapse Study Type: Phase III Cardiovascular Site Type: Government Academic Institution Problem: Major audit finding regarding IP temperature excursions. Root Cause: The site claimed to have 24/7 power backup but did not have a dedicated, monitored power line for the IP refrigerator. Action Taken: All subjects at the site were excluded from the primary analysis. Outcome: Compromised data integrity and a significant delay in the NDA submission. Lesson Learned: Physical verification of infrastructure and backup logs is non-negotiable during the Site Selection Visit (SSV). Case Study 3: The Ethics Committee Quagmire Study Type: Rare Disease / Orphan Drug Site Type: Specialist Tertiary Care Center Problem: 7-month delay in start-up. Action Taken: Sponsor had to wait for the site to re-register the EC. Outcome: Missed the global recruitment window for the first cohort. Lesson Learned: Verify the EC’s CDSCO registration status and expiration date before finalizing the site. Case Study 4: Data Quality and ALCOA+ Violations Study Type: Biosimilar Comparison Site Type: Private Research Site Problem: Systematic errors in source documentation. Root Cause: No dedicated Quality Management System (QMS) at the site level; staff was using “shadow files” instead of real-time entry. Action Taken: Intensive retraining and 100% Source Data Verification (SDV). Outcome: Monitoring costs tripled for this specific site. Lesson Learned: Assess the site’s internal SOPs for data management during feasibility, not just their patient numbers. Challenges and Mitigation Strategies Sponsors frequently underestimate the complexity of logistics in India. For example, shipping laboratory samples across state lines or ensuring cold chain integrity in high-heat zones requires more than a standard courier. Instead, sites must use specialized logistics systems designed for temperature-sensitive clinical materials. As a result, sample quality and data reliability can be consistently maintained.Mitigation starts with honest site assessment. For instance, if a site lacks experience with the specific therapeutic area or the diagnostic equipment required by the protocol, it must be disqualified, regardless of its reputation. Therefore, sponsors should prioritize operational capability over brand recognition. As a result, study quality and protocol compliance are better protected. We often recommend using a dedicated Site Management Organization (SMO) to bridge the gap between the PI’s clinical expertise and the trial’s operational requirements. For more information on how to navigate these complexities, visit our clinical research services India page. Myths vs Reality in Indian Clinical Trials Reality: Patient volume is useless if the
